
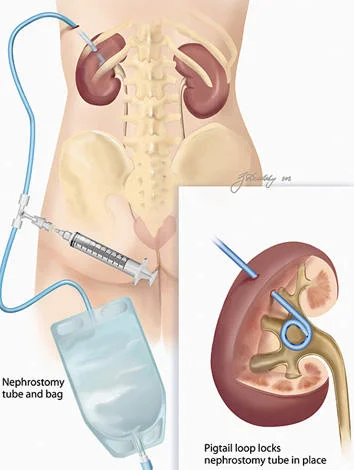
Nephrostomy Tube
A nephrostomy tube is the term used for a catheter that perforates the skin and abdominal cavity ultimately being placed into the renal pelvis or calyx. There are different situations which arise that may require access to the kidney by this method. Patients may need to have two nephrostomy tubes placed if both kidneys are compromised.
Indications
There are certain types of situations in which a nephrostomy tube is indicated. Although this seems like a very straightforward procedure, it can be lifesaving in certain situations. Medscape states that there are number of indications for a nephrostomy tube:
Acute or chronic upper urinary tract obstruction in which access to the kidney is impossible from the lower urinary tract because of stones, infections, tumors, or anatomic anomalies, especially when a double-J stent cannot be placed through the ureter because of above-mentioned circumstances
When a patient's creatinine level is rising above the reference range and the urine cannot be drained through the ureter
Renal pelvis disorders (eg, UPJ obstruction, horseshoe kidneys, ureter duplex, ureter fissures, double renal collecting systems)
Hydronephrosis in renal transplant allografts: When dilatation of the renal pelvis affects kidney function to the extent that double-J stent placement is difficult or impossible, percutaneous nephrostomy may be an easier option.
Treatment of staghorn calculi and large or lower-pole kidney stones (when a percutaneous nephrolithotomy [PCN] is likely to be followed because of the stone burden and an extracorporeal shockwave lithotripsy [ESWL] is less likely to be successful)
Contraindications to ESWL (ie, size of patient): Most ESWL units have a weight limit of 140 kg (approximately 300 lb).
Body habitus that prevents ESWL (eg, contractures): Disabled patients occasionally cannot be positioned on an ESWL unit in a prone or supine position.
Stones or tumors associated with distal obstruction or a foreign body that cannot be removed through the ureter
When rapid dilation of the nephrostomy tract is required (eg, when access is needed instantly for operative procedures within the renal collecting system [for stone removal or tumor ablation])
Prolonged sequential dilatation: Gradually increasing the catheter size may be necessary when a nephrostomy tube is placed permanently for urine drainage in patients in whom a retrograde access to the kidney is impossible (eg, advanced metastatic tumors, loss of the total ureter, patients with a palliative nephrostomy tube whose cases are inoperable).
A rare indication is antegrade nephrostomy to control a ureteral lesion after ureteral trauma that cannot be fixed in a retrograde fashion in a nonobstructed kidney. This can occur with a completely dissected ureter after gynecological, surgical, or urological procedures discovered after the procedure. Most likely, a urinoma has developed around the dissected ureter, with the kidney itself not being obstructed but in being need for a nephrostomy.
In an emergency situation a nephrostomy may always be mandatory.
Other relevant articles include:
Resources





